
Clinical Mind AI: A More Scalable Way to Teach Clinical Reasoning
A Stanford-born platform uses a custom GPT to help health professions instructors build low-cost, multilingual clinical simulations in minutes.

Source note: This is an edited interview adapted from a narrated video demo by Dr. Marcos Rojas.
Marcos Rojas, MD, is a physician from Santiago, Chile, and a Ph.D. candidate at Stanford University’s Graduate School of Education focused on advancing medical education. His work explores innovative uses of technology to enhance clinical training, and he serves as the Project Director of Clinical Mind AI.
Intro
Clinical simulation is one of the most powerful ways to teach clinical reasoning. It gives students a chance to practice the messy, high-stakes work of listening, asking better questions, forming hypotheses, and deciding what to do next before a real patient is in front of them.
But simulation is hard to scale. High-fidelity simulations require actors, equipment, space, and trained staff. Even virtual simulations can be difficult to adapt because they are often built in English, tied to one health system, or too rigid for local curricula.
Clinical Mind AI started with a narrower question: could a custom GPT simulate a realistic conversation with a patient? That proof of concept led to a larger one: what if generative AI could support the full workflow of simulation-based teaching, from case creation to student feedback?
In this interview, Dr. Marcos Rojas, Project Director of Clinical Mind AI, explains how the platform began, how it works, and why scalable simulation could matter for health professions education around the world.
The Interview
Q: What’s the problem you were trying to solve when this began?
Dr. Marcos Rojas: Simulation is a powerful tool for teaching clinical reasoning, but it is often costly and hard to scale. Many institutions, especially in low-resource settings, do not have access to high-fidelity simulation centers. That means students in medicine, nursing, pharmacy, dentistry, and other health professions may not get enough opportunities to practice the complex reasoning they will need with real patients.
The problem is not just access. It is adaptability. Many virtual simulations are designed in English, built around a specific health system, and difficult to localize. We wanted something instructors could adapt to their own context.
Q: What was the first experiment?
Dr. Marcos Rojas: At Stanford, we began with a simple custom GPT that simulated a conversation with a patient. A learner could ask the AI patient questions, and the patient would respond with realistic, medically coherent answers.
That first version showed us something important: generative AI could replicate the feel of a live patient encounter. It was exciting, but it was also limited.
Q: Limited in what way?
Dr. Marcos Rojas: Instructors wanted more than a patient chatbot. They wanted to create cases quickly, adapt cases to their own clinical and cultural context, give students feedback, include visuals such as pictures or x-rays, and even support voice or phone-style interactions.
That pushed us to ask a broader question: what if generative AI could power the entire workflow of simulation-based teaching?
Q: So what is Clinical Mind AI now?
Dr. Marcos Rojas: Clinical Mind AI is a web-based platform that helps instructors build and run AI-supported clinical simulations. Several parts of the platform use a GPT model, other generative AI models, and additional AI techniques.
For case creation, instructors provide details and learning goals. AI helps refine the case, adapt it to cultural and system context, and check plausibility. During simulation, a GPT model powers real-time medically realistic conversations with AI patients. For feedback, AI reviews the interaction transcript and highlights strengths and areas for improvement based on the instructor’s objectives and rubrics.
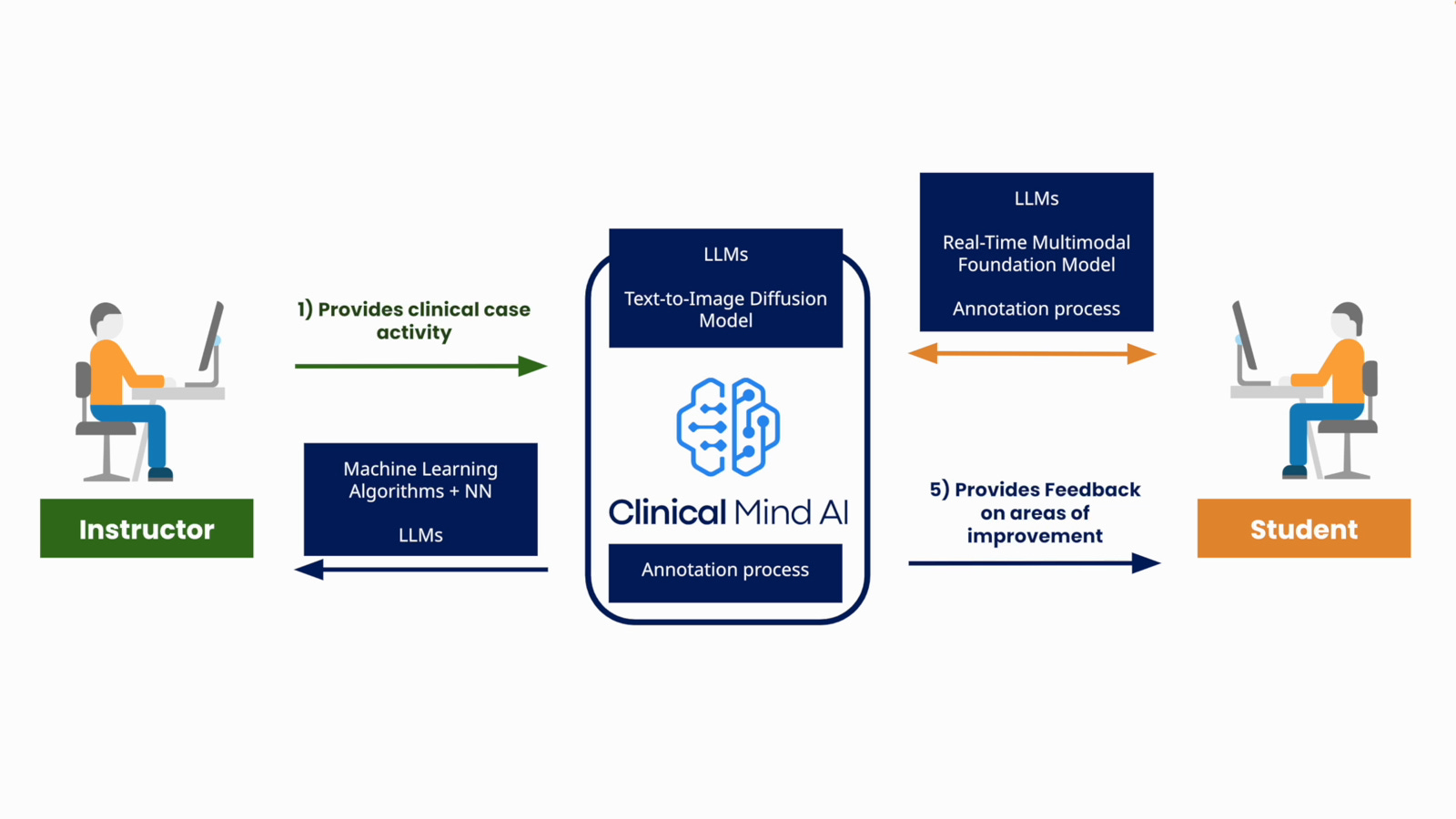
The platform connects instructor-authored activities, AI-supported patient interactions, and student feedback.
Q: What is the design principle underneath that workflow?
Dr. Marcos Rojas: The design principle is that instructors should be able to move from an idea to a ready-to-run simulation in minutes, without coding, technical setup, or juggling multiple tools.
Under the hood, the platform makes multiple API calls to the model most appropriate for each function. The GPT model can handle dialogue for the simulation. Other generative text models support case creation and feedback. An image generation model can produce realistic, non-identifiable patient visuals.
This multi-model architecture gives us flexibility and scalability. It also lets us upgrade pieces of the system as better models become available.
Q: Walk me through what an instructor actually does.
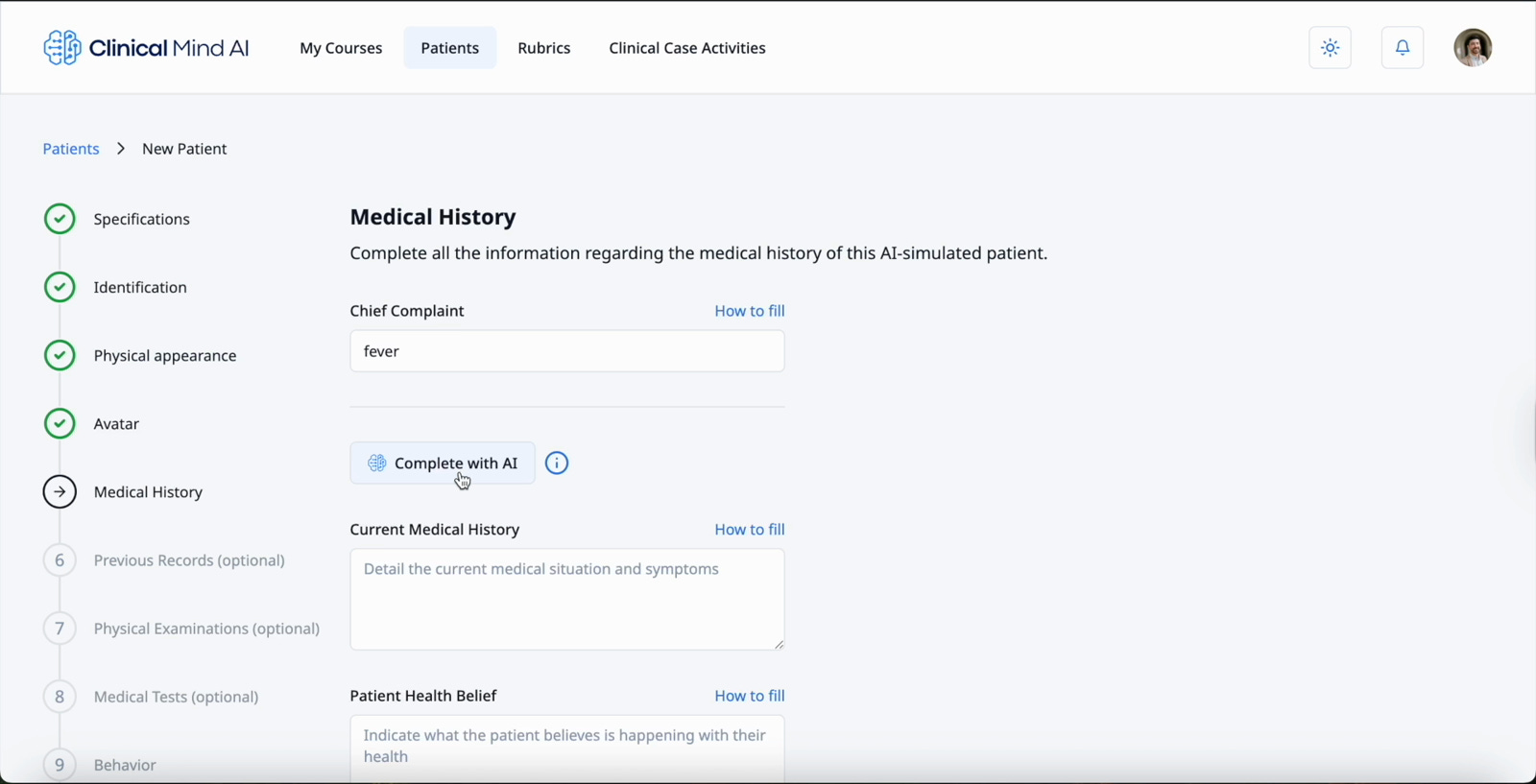
Dr. Marcos Rojas: When instructors log in, they start inside a course. From there, they can create AI-simulated patients. They fill out a form with patient details: name, chief complaint, physical examination, and any other information that belongs to that patient.
They can also generate or select a patient avatar. The point is not decoration. The image helps the case feel more realistic while staying non-identifiable and matched to the case description.
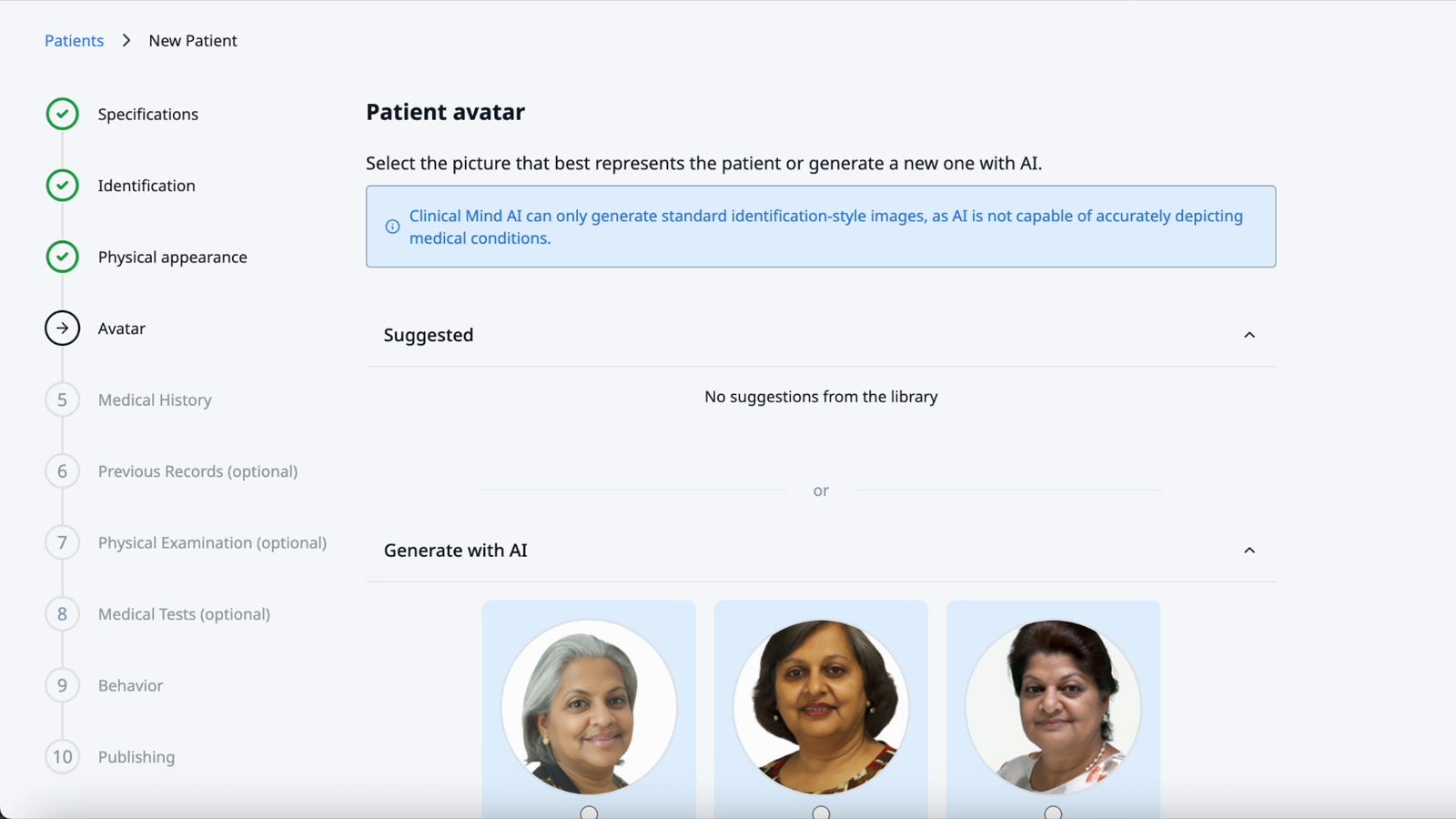
Instructors can use AI-generated, non-identifiable patient visuals to add realism to a simulation.
Q: How does feedback work?
Dr. Marcos Rojas: If instructors want students to receive feedback, they create rubrics. Those rubrics can be applied to open-ended answers or to interactions where students talk with the patient, request a physical examination, or ask for medical tests.
The rubric gives the AI a standard to evaluate against. Feedback is not generic. It is tied to the instructor’s objectives and to the criteria they put into the system.
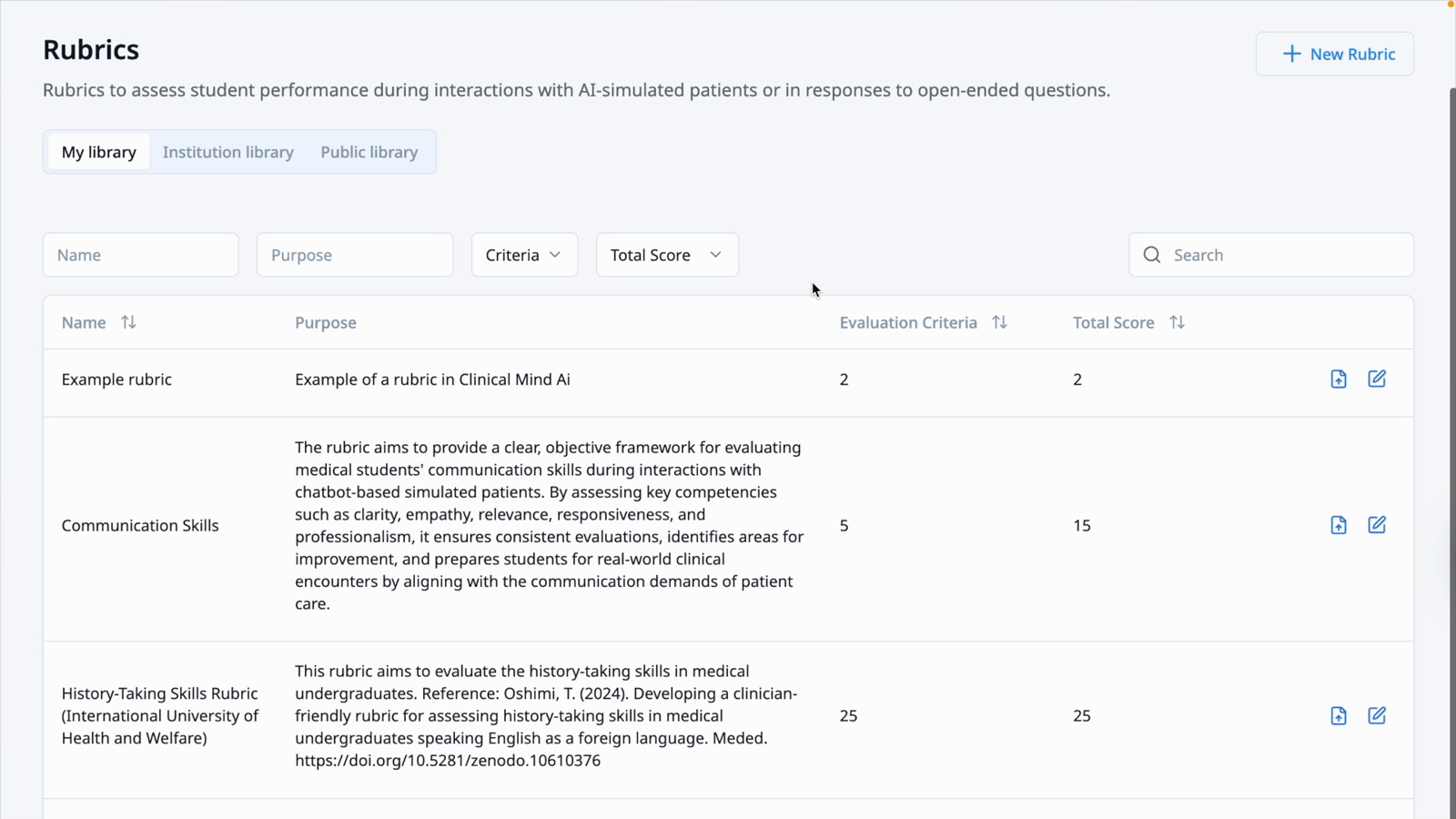
Rubrics let instructors define the criteria used to evaluate student responses and patient interactions.
Q: What happens after the patient and rubric are ready?
Dr. Marcos Rojas: The instructor creates a Clinical Case Activity. This is where they combine the pieces into the sequence students will experience.
For example, a student might first talk to the patient. Then they answer a question. Then they request a physical examination. After that, the instructor can add another question, a media file, or another activity step. The instructor can make the sequence short or long, simple or complex.
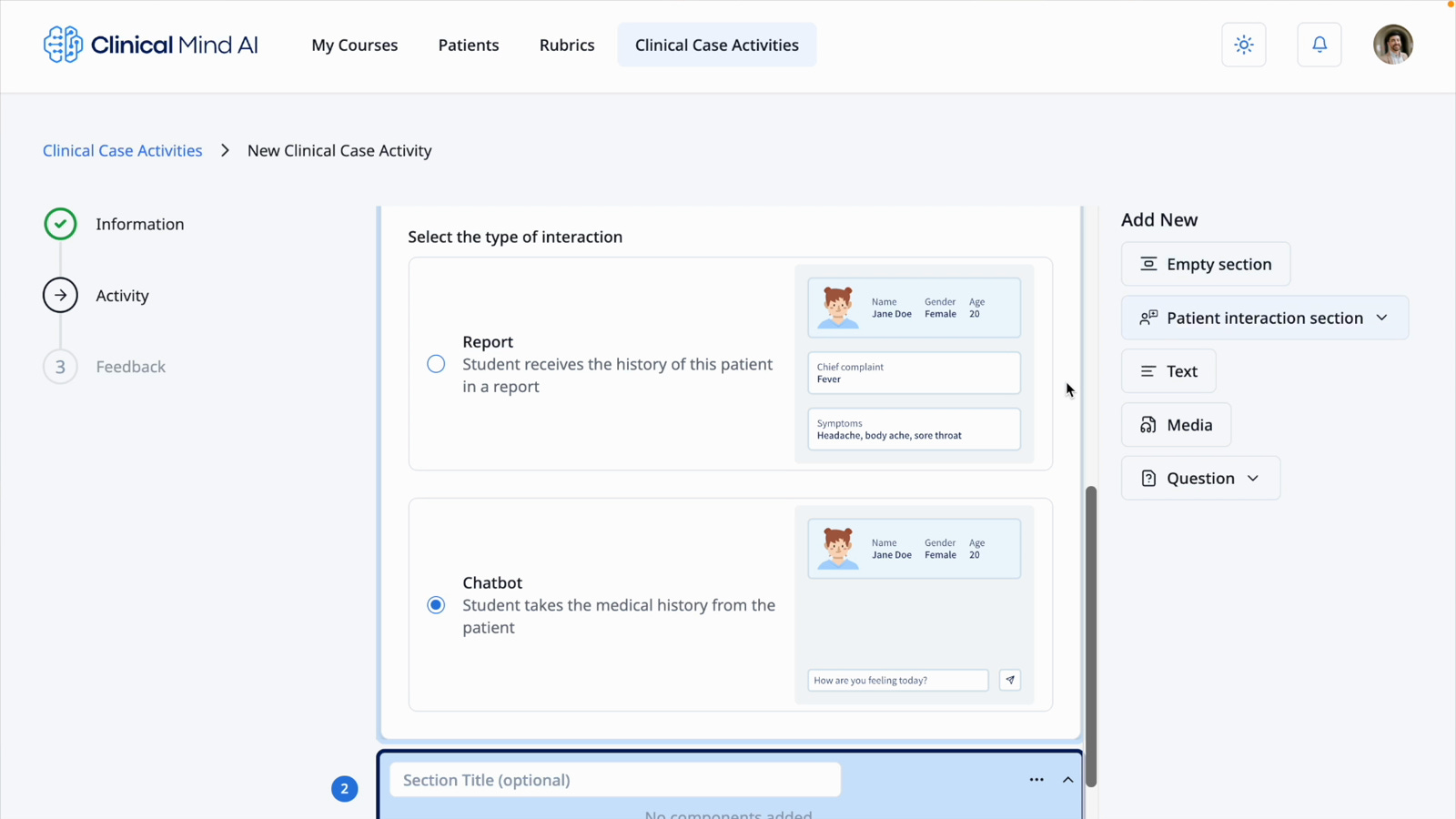
A Clinical Case Activity can combine chatbot interactions, questions, media, and feedback into one student-facing sequence.
Q: What changes for students?
Dr. Marcos Rojas: Students log into the platform and follow the sequence their instructor created. If feedback is enabled for the activity, they receive feedback based on the instructor’s rubric.
The goal is a more realistic, adaptive environment for practicing clinical skills. Instead of only reading a static case, students can interact with a patient, make requests, answer questions, and receive targeted feedback.
Q: What changes for institutions?
Dr. Marcos Rojas: Each simulation costs only a few cents to run. There is no need for actors, equipment, or simulation centers.
Because the platform is multilingual and curriculum-agnostic, it can be integrated into health professions programs in many different settings. That is especially important for institutions that do not have much access to simulation centers but still want students to practice rich, interactive scenarios at scale.
Q: What evidence do you have so far?
Dr. Marcos Rojas: Clinical Mind AI started as a small project at Stanford, but it quickly resonated with educators beyond campus. Today, 21 universities are part of the platform, with more about to join.
We piloted Clinical Mind AI in one Stanford course. We also completed a first research project on feasibility and acceptability involving 51 medical instructors across the United States. Other research projects are underway, including work on learning impact, AI-powered feedback, and additional features to support instructors globally.
Early signals from the work include:
Case creation: Reduced from hours to minutes.
Instructor feedback: 51 medical instructors included in feasibility and acceptability research.
Adoption: 21 universities are part of the platform, with more expected.
Student experience: Students report higher immersion and motivation than with static case-based scenarios.
Institutional value: Low-resource institutions can run interactive simulations at scale.
Q: The “hours to minutes” claim is striking. What makes that possible?
Dr. Marcos Rojas: One example is the Generate the Case feature. When instructors are filling out a clinical case form, they can click Generate the Case. Generative AI fills out the form quickly, giving instructors examples they can edit instead of forcing them to write everything from scratch.
That changes the work. The instructor is still the expert, but they are revising, adapting, and checking a generated draft rather than starting from a blank page.
Generative AI can help pre-fill clinical case details, shifting instructors from blank-page writing to expert review and adaptation.
Q: What has made the project possible?
Dr. Marcos Rojas: The platform has grown through the combined perspectives of educators, engineers, developers, researchers, professors, and institutional collaborators at Stanford University and around the world.
Each group brings a different lens: designing cases, refining AI outputs, and integrating the tool into local curricula. That diversity of perspectives and motivations is what makes the project possible.
Q: What’s the larger ambition?
Dr. Marcos Rojas: The goal is to help instructors drive educational innovation and make sure students, regardless of location or resources, can develop essential clinical skills in a realistic, adaptive environment.
By combining AI with the creativity and expertise of doctors, educators, engineers, professors, and collaborators across the globe, we believe we are shaping a more equitable future for health professions education.
Closing
The promise of Clinical Mind AI is not that AI replaces clinical educators. It is that AI can help educators create more practice, more context, and more feedback for more learners.
The core question is no longer just whether an AI patient can hold a believable conversation. It is whether the whole simulation workflow can become easier to build, easier to adapt, and available to students who would otherwise have far fewer chances to practice.
About Dr. Marcos Rojas
Marcos Rojas, MD, is a physician from Santiago, Chile, and a Ph.D. candidate at Stanford University’s Graduate School of Education focused on advancing medical education. His work explores innovative uses of technology to enhance clinical training, and he serves as the Project Director of Clinical Mind AI.
Very interesting! I was immediately hooked by the “clinical” part.
I’m curious how the Clinical Mind AI integrates with existing AI tools. Does it mainly live within its own platform, or is it also accessible through ChatGPT, Claude, and similar interfaces?
The useful line here is the shift from static case content to a closed loop: attempt, transcript, rubric, feedback, next attempt. In surgical training, that boundary matters because a simulation only becomes training when the feedback changes the next repetition.